

If you are reading this on your phone, pause for a minute. Look at your back in the mirror or ask someone to check it. Do you see a spot you had not noticed before?
If not, good. If yes, do not panic: in most cases it is nothing serious. But it is precisely the small percentage of cases that people ignore that explains why more than 2,400 new cases of melanoma are recorded in Ukraine every year, and around 840 patients die from it. The worst part: almost half of patients come in already at stage II because they “did not pay attention.”
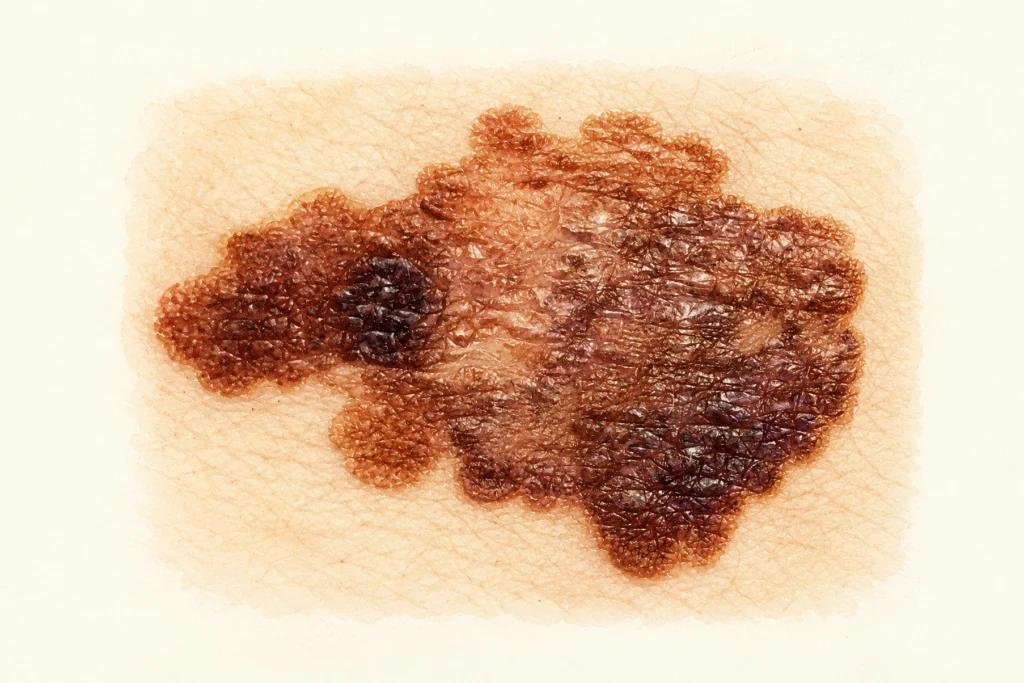
Most articles about moles talk about the ABCDE rule. It is useful. But it does not cover every type of melanoma: nodular, acral, or subungual melanoma may not look like the classic dark, asymmetric mole — and these account for up to one third of all cases. This article explains what is usually left out: where melanoma hides, what ABCDE does not detect, and what modern dermatological screening looks like.
The ABCDE rule: essential, but not enough on its own
ABCDE is the international alphabet of signs to look for during self-examination. Five letters, five criteria.
| Letter | What it means | What to look at | Warning sign |
| A — Asymmetry | Asymmetry | Mentally divide the mole in half — the two halves should mirror each other | One half is “longer,” or has a different shape or color |
| B — Border | Border | A healthy mole usually has clear, even borders | The borders are uneven, map-like, blurred, or jagged |
| C — Color | Color | One or two shades of brown are usually normal | Three or more colors: brown + black + red, white, or blue |
| D — Diameter | Diameter | The classic threshold is over 6 mm — about the size of a pencil eraser | Any spot larger than 6 mm, although “mini-melanomas” of 3–4 mm also exist |
| E — Evolution | Evolution | Any change over weeks or months | A change in shape, color, or size, or the appearance of itching or bleeding |
The letter E is the most important one. A mole that has remained stable for 20 years usually does not turn into melanoma within a week. But any change is a reason to schedule an examination.
ABCDE works well for superficial spreading melanoma — the most common subtype. It accounts for about 70% of all cases. Some melanomas do not have the full set of classic ABCDE signs, so self-examination should not be limited to this rule alone. These include two particularly concerning subtypes: nodular and acral melanoma. They are the ones most often missed, and they are also among the most likely to be fatal.
The EFG rule: what ABCDE does not catch
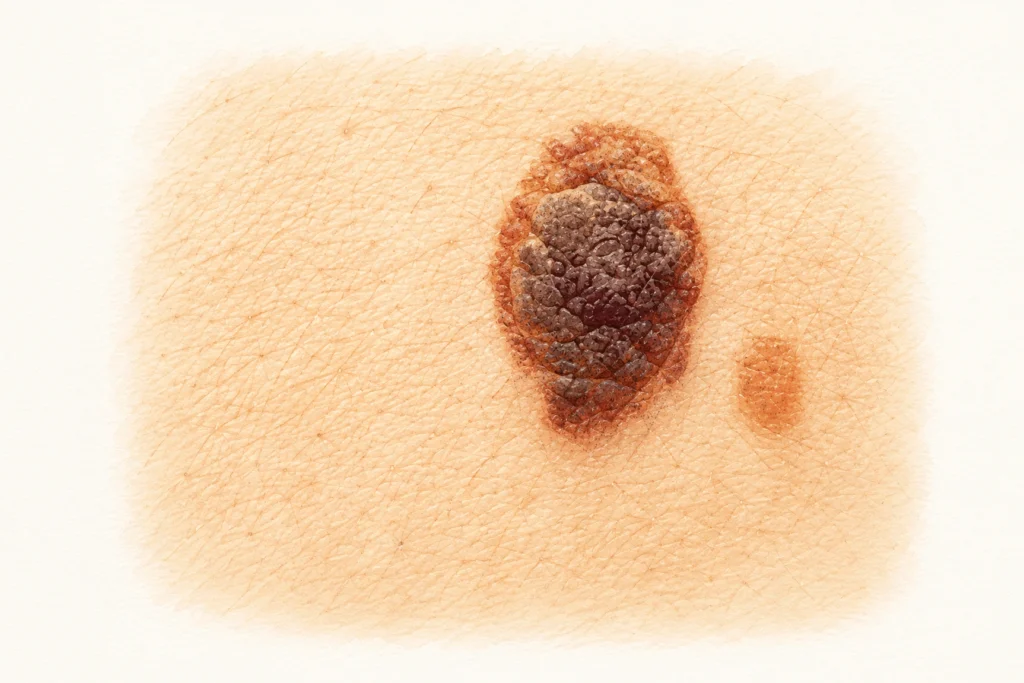
Nodular melanoma is the most aggressive subtype. It grows not across the surface, but deeper into the skin, so even a small nodule can become life-threatening within a few weeks. It accounts for 15–20% of all melanomas, but it is responsible for most melanoma deaths at a young age.
An important detail: it often does not look like a “classic scary mole.” It may be symmetrical, have a smooth border, and be a single color. In 50% of cases, it is not dark, but pink, red, or skin-colored — like an ordinary pimple or boil that “does not go away.”
That is why dermatologists added another rule to ABCDE — specifically for nodular melanoma. It is called the EFG rule.
| Letter | What it means | What it looks like in real life |
| E — Elevated | Raised above the skin | Not a flat spot, but a clearly raised bump or nodule |
| F — Firm | Firm to the touch | Press it with your finger — it does not “soften” like a pimple, but feels elastic, like a firm rubber eraser |
| G — Growing | Increasing in size | A noticeable change over 2–6 weeks, not over years |
The rule is simple: if you have developed a “pimple” that has not disappeared within a month but has instead grown and become firmer, do not rule out melanoma just because it is not dark. Show it to a doctor.
The “ugly duckling” sign: when a mole does not fit the pattern
Each person has their own group of moles on the body. Usually, they are similar in shape, size, and shade. This is biology: all moles arise from similar cells, so within one body they tend to have the same “style.”
A suspicious mole is one that stands out from this pattern. Darker than all the others, or, on the contrary, lighter. Larger. A different shape. The “ugly duckling” sign is not a formal criterion measured in millimeters. It is an intuitive feeling that “something is not right.”
Interestingly, this sign is often noticed by close people rather than by the patient. A husband notices something on his wife’s back; a hairdresser spots something on a client’s scalp. If someone around you thinks your mole is “not like the others,” it is worth checking.
Blind spots: where melanoma is most often missed
Most patients examine their face, chest, and forearms. The rest of the body — rarely or never. But melanoma often appears exactly where no one looks. Let us review these areas.
Scalp
Melanoma on the scalp is rare, but it has the highest mortality compared with melanomas in other locations — it is noticed late because it is hidden under the hair. Once a month, part your hair with a comb and check the scalp — preferably in front of a mirror and in good lighting. This is especially important for people with thinning hair or early balding. Your hairdresser can also be a useful ally. Ask them to tell you if they notice a new dark spot, a crust that does not heal, or a mole that has changed.
Feet and the spaces between the toes
Acral melanoma is a subtype that is not linked to sun exposure. It develops on the palms, soles, and under the nails — areas that are almost never exposed to the sun. It is often mistaken for a callus, wart, or fungal infection. When examining your feet, pay attention not only to the soles but also to the spaces between the toes. This is especially important for people with diabetes, as their feet should already be checked regularly.
During dermoscopy of acral areas, there is a specific sign that can be seen only under magnification: melanoma lies on the ridges of the skin markings, while a benign mole lies in the furrows themselves. This is one reason why a spot on the foot is a reason for dermoscopy, not for self-monitoring.
A dark stripe under the nail
This is a separate issue that very often ends in a late diagnosis. A dark longitudinal stripe under the nail may be:
- the result of trauma — a hematoma, which is the most common option
- a benign nevus of the nail matrix
- subungual melanoma — rare, but life-threatening.

How can you tell the difference? A hematoma moves upward over time as the nail grows — within 3–6 months it “grows out” toward the edge and disappears. Melanoma does not move. The second important sign is the Hutchinson sign: pigmentation spreads from under the nail onto the surrounding skin, the nail fold. This is almost always a warning sign.
There is also so-called pseudo-Hutchinson sign — when the pigment under the nail simply shows through the thin skin of the nail fold, but does not actually extend beyond the nail plate. Only dermoscopy can tell the difference.
If a dark stripe under the nail does not disappear within 6 months, is wider than 3 mm, or spreads onto the skin near the nail, this is a reason for urgent examination.
Palms
There are usually few moles on the palms, so any new dark spot needs to be checked. Especially if it has an irregular shape or is changing.
Back
The back is the most common area where melanoma is detected late — simply because the patient cannot see it. This requires two mirrors — one large and one handheld — or help from a partner. A partner-assisted check every 1–2 months significantly increases the likelihood of early diagnosis, as confirmed by international studies.
Oral mucosa
Yes, melanoma can occur there too — on the hard palate, gums, and, less often, the tongue. This subtype is rare, but its prognosis is much worse than that of cutaneous melanoma because it is diagnosed late. Unlike on the skin, ABCDE does not work for mucous membranes, and there are no simple criteria for oral self-examination. Any new dark spot in the mouth, noticed by you or during a dental check-up, is a reason for consultation.
The dental specialization of H-Clinic works in the patient’s favor here: in our clinic, a dermatologist and a dentist work under one roof, so the skin and oral mucosa can be examined during one visit.
Genitals
Melanoma in this location is rare. This does not mean you need regular self-examination with a magnifying glass — it is enough to pay attention to any new dark spots that have appeared and do not go away. If you have questions, it is better to discuss them with a gynecologist, urologist, or dermatologist — and not postpone the visit because of embarrassment.
Warning signs by body area
| Area | Usually not alarming | Red flag | What to do |
| Scalp | An old mole present since youth | A new spot; a crust that has not healed for more than 3 weeks | Check the scalp by parting the hair every month |
| Palms | Freckles, calluses | A new dark spot over 3 mm with an irregular border | See a dermatologist |
| Feet and between the toes | Calluses, cracks | A spot that does not disappear; a new dark spot | Check monthly |
| Under the nail | Hematoma — moves as the nail grows over 3–6 months | A dark stripe that does not move; pigment spreading onto the skin of the nail fold | See a dermatologist urgently |
| Back | Old, stable moles | Any new asymmetric spot over 5 mm | Partner check + photo documentation |
| Oral mucosa | Natural pigmentation; dark areas near old amalgam fillings | A new dark spot on the gums or palate | See a dentist or dermatologist |
| Genitals | Naturally darker areas | A new spot with an irregular border or one that bleeds | See the relevant specialist |
Amelanotic melanoma: when “nothing dark” does not mean safe
About 2–8% of melanomas have no pigment. They are pink, red, or skin-colored. Doctors call them “great masqueraders”: they look like a pimple, irritation, or a small wound that just does not heal.
Most patients ignore such lesions for a long time precisely because they have the idea “melanoma = dark spot” fixed in their mind. And by the time the lesion finally becomes something that clearly no longer looks like a pimple, several months may have passed — and these are often months of lost time.
A simple rule: if there is something on your skin that looks like a sore, ulcer, or bump and does not heal for more than 4 weeks, show it to a doctor. Even if it is not dark.
Benign “look-alikes” of melanoma: what you usually do not need to fear
Alarming thoughts are easy to sell. But the truth is that most skin lesions patients come in with are benign. It is useful to know what they look like: both to worry less and to avoid confusing them with truly dangerous lesions.
| What it is | What it looks like | Is it dangerous? | What to do |
| Seborrheic keratosis | A “stuck-on” brown plaque, as if attached to the skin; appears with age | No | It can be left alone; removed for cosmetic reasons |
| Dermatofibroma | A small firm bump; when squeezed from the sides, it seems to “dimple” into the skin | No | Observe |
| Solar lentigo | Flat brown spots on the backs of the hands, face, and shoulders | No — but it is a marker of photoaging | Laser treatment if desired |
| Cherry angioma | A bright red dot, like a drop of wax | No | Laser treatment if desired |
| Blue nevus | A dark blue dot, well-defined and round | Usually no | Dermoscopy for reassurance |
| Atypical — dysplastic — nevus | Larger and more irregular than a typical mole, but flat | Increased risk in people with 5+ such moles | Monitor, with photo documentation |
A small nuance that practitioners know: seborrheic keratosis can sometimes look like melanoma even to an experienced eye — and the reverse can also happen, when melanoma mimics seborrheic keratosis. So “it does not look scary” is a hypothesis, not a diagnosis. Dermoscopy helps the doctor assess the lesion, while in doubtful cases, the final answer is provided by histology.
Who is at risk and how often to get checked
Not everyone needs an annual dermatologist check-up. The frequency depends on your risk factors. The main ones are:
- fair skin that tans poorly — Fitzpatrick skin types I–II
- blond, red, or light brown hair
- blue, green, or gray eyes
- freckles, especially on the shoulders and back
- sunburns in childhood, especially blistering sunburns
- more than 50 moles on the body
- the presence of atypical moles
- melanoma in close relatives
- immunosuppression — organ transplantation, immunosuppressive therapy, chemotherapy
- a personal history of melanoma or another skin cancer.
| Risk group | Who this includes | Self-examination | Dermatologist examination | Digital mole mapping |
| Low | Darker skin, up to 20 moles, no significant history | Once a month | Once every 2–3 years | Not needed |
| Moderate | Fair skin, freckles, childhood sunburns | Once a month | Once a year | Optional |
| High | 50+ moles, atypical nevi, melanoma in the family | Once a month | Every 6 months | Recommended |
| Very high | Personal history of melanoma, hereditary syndromes, immunosuppression | Once a month + partner-assisted check | Every 3–4 months | Required |
What a professional examination looks like
Professional dermatological screening takes 20–40 minutes and consists of several stages.
Medical history. The doctor asks about your skin phototype, family cancer history, childhood sunburns, previous skin lesions, and medications. If this is your first visit, allow time for a detailed conversation and do not rush.
Full-body examination. This means literally the entire body: from the scalp to the spaces between the toes, including the nails, intertriginous areas, and genitals. It may sound uncomfortable, but it is the standard. An examination only of “the area that bothers you” is not screening, but a consultation for a specific concern.
Dermoscopy of suspicious areas. This is performed with a device that uses magnification and polarized light to show the internal structure of a mole at a level unavailable to the naked eye. It is painless, non-invasive, and takes only a few seconds per lesion.
Digital mole mapping — for high-risk and very-high-risk patients. The entire surface of the body is photographed in standard positions; individual suspicious lesions are documented in dermoscopic mode, and the data are stored in a digital archive. At the next examination, after 3–12 months, the images are compared — the software detects new and changed moles.
Biopsy if a malignant lesion is suspected. Excision of the entire lesion followed by histological examination is the gold standard. Partial biopsy of a mole is not recommended because it changes the structure of the lesion and makes diagnosis more difficult.
At H-Clinic, the examination is performed by a dermatologist experienced in dermoscopy; if needed, you can also consult a dentist about the oral mucosa during the same visit — without a separate appointment or repeat visit.
How to document moles with photos at home
Photos are useful, but often used incorrectly as a self-monitoring tool. A few rules can make photo documentation truly effective.
Lighting. Diffused daylight, preferably near a window. Not a phone flashlight, not a ceiling light, and not light from a screen.
Background. Plain, preferably light-colored. A sheet, a piece of paper, or a bathtub.
Distance. Take two photos of each suspicious mole: a general photo of the body area — so it is clear exactly where the mole is located — and a close-up from a distance of 10–15 cm.
Ruler. Place a school ruler or a special measuring sticker next to the mole. Without scale, comparing size over the months will be inaccurate.
Frequency. If you have many moles — once every 3 months. If you have few moles and are in a low-risk group — once a year.
What to compare. Size, shape, color, and the appearance of new lesions.
What not to do. Do not rely on photos alone. They do not replace dermoscopy. They are a tool between scheduled visits, not a substitute for them.
Mole-checking apps: an honest assessment
A question we are asked regularly: can apps such as SkinVision, MoleScope, and similar tools be trusted? It depends on how you use them.
The accuracy of such apps in real-life conditions ranges around 70–90% in terms of sensitivity — how well they detect true melanomas — and is lower in terms of specificity — how well they avoid false alarms. In other words, an app can both miss melanoma and scare you unnecessarily.
As a tool between doctor visits, apps can be useful. As a replacement for a doctor — no. If an app shows a red warning, go for dermoscopy. If it shows green, that is not a guarantee either. No neural network has yet replaced the trained eye of a dermatologist with a dermatoscope.
Quick checklist
- Look at your palms and feet, including the spaces between your toes.
- Check your nails — look for any dark stripe under the nail plate.
- Set a reminder on your phone for a self-examination in one month.
- If you find something that worries you, schedule an examination this week, not “later.”
Conclusion
Dermatological screening is not a reason to be afraid, but a skill that helps detect danger in time. Most spots patients come to the clinic with turn out to be harmless. But the skill of telling “harmless” apart from a real threat takes 15 minutes of attention per month — and one examination per year.
If you have spots that worry you, or if you simply have not had a routine check-up for a long time, our dermatologists will perform a full dermoscopic screening with digital mapping if needed. It is better to make sure everything is calm one extra time than to be late.
Frequently asked questions
If a mole has not changed for 20 years, does that mean it definitely does not need to be touched?
If it is stable in all parameters — size, color, shape, and surface — and does not bother you, then most likely not. Stability for 5+ years is strong evidence of benignity. But “stable for 20 years” does not mean “unchangeable for life.” It is still worth showing it once a year.
I developed a new mole at the age of 35–40. Is this normal?
The appearance of new moles after the age of 30–35 becomes less typical, and after 40 it should raise attention. This does not mean the mole is necessarily dangerous, but it is a reason for dermoscopy. The older the age, the more carefully new lesions should be assessed.
Is it true that an injured mole will definitely turn into melanoma?
No, this is a myth. A one-time injury — a cut or scrape — does not in itself “turn” a mole into melanoma. Long-term repeated trauma to a mole over many years is a different matter, for example from a bra strap or a belt. In such cases, removal for cosmetic and preventive reasons may be justified.
Will removing moles “just in case” help prevent melanoma?
No. In 70–80% of cases, melanoma develops not from old moles, but on clear skin. So “removing everything” is not a prevention strategy. Lesions that are clinically or dermoscopically suspicious, or those that are constantly traumatized, should be removed. The rest should be monitored.
Laser or surgery — which removal method is safer from an oncologic standpoint?
The key difference is this: during surgical removal, the lesion is removed whole and sent for histological examination. During laser removal, the tissue is vaporized, so it can no longer be examined under a microscope. If there is even the slightest suspicion of malignancy, only surgery with histology is appropriate. Laser removal is acceptable only for moles that the doctor is completely confident are benign.
Can moles be removed during pregnancy?
Planned removals for cosmetic reasons are usually postponed until after childbirth and the end of breastfeeding. But if a mole has changed or a new suspicious one has appeared, diagnosis and removal are performed regardless of pregnancy. Modern anesthesia and surgical techniques are safe for the fetus. Delaying removal of a suspicious lesion for 9 months is more dangerous than removing it.
Is dermoscopy painful? How often should it be performed?
It is completely painless. The doctor places a device that looks like a small microscope against the mole and examines it through the device. Contact with the skin is minimal, with no discomfort. Frequency ranges from once every 2–3 years for people at low risk to once every 3–4 months for patients at very high risk.
What should I do if I cut a mole with a razor or it starts bleeding?
Stop the bleeding, apply an antiseptic, and monitor it. If it is a one-time cut and the mole was not suspicious, this is usually not dangerous. But if a mole bleeds on its own, without an obvious reason, this is a red flag — see a doctor that same week.
Can mole-checking apps be trusted?
They can be useful as a tool between doctor visits. As a replacement for a doctor — no. Their accuracy is around 70–90%, meaning they miss some melanomas and produce false-positive alerts. A red alert in an app is a reason to see a dermatologist. A green result is not a guarantee.
A child has developed new moles. Is this a reason for an examination?
The appearance of moles in childhood and adolescence is normal. Most moles in children are benign. You should be concerned if a mole grows quickly, stands out from the others, is constantly traumatized, or was present from birth and has enlarged. In that case, the child should be examined by a pediatric dermatologist.
Is a dark stripe under the nail a trauma mark or a reason to worry?
Most often, it is a hematoma after an injury, even if you do not remember the injury. As the nail grows, a hematoma moves upward and grows out within 3–6 months. If the stripe does not move, is wider than 3 mm, becomes darker, or spreads onto the skin around the nail, an urgent examination by a dermatologist is needed. It may be subungual melanoma.
Can melanoma appear in the mouth?
Yes. This is a rare subtype, but it does exist — on the hard palate, gums, and, less often, the tongue. The prognosis is worse than for cutaneous melanoma because it is diagnosed late. Any new dark spot in the oral cavity, noticed by you or by a dentist, is a reason for consultation. We are preparing a separate article about oral melanoma.
How can I know that a mole was removed correctly — and is histology always required?
Histology is required after any removal of a pigmented lesion. Without it, you do not know exactly what was removed. The pathologist’s report should include: the type of lesion, whether there are signs of atypia or malignancy, and whether the excision margins are clear. Keep this report — it is your medical document for life.
Is it safe to sunbathe if I have many moles?
The more moles you have, the higher your baseline risk of melanoma, and the more carefully you should treat sun exposure. This does not mean “no sun at all.” It means: avoid peak sun hours — from 11:00 to 16:00 — use SPF 30+ sunscreen on exposed areas, wear a wide-brimmed hat, and stay in the shade during peak hours. There is no need to “cover” individual moles separately — protect all of your skin as a whole.
Can melanoma appear on an area that has never been exposed to the sun?
Yes. Acral melanoma — on the palms, soles, and under the nails — is practically unrelated to ultraviolet radiation. Mucosal melanomas — in the mouth and genital tract — are also unrelated. In people with darker phototypes, melanoma more often develops in these exact areas. This breaks the common myth: “I do not sunbathe, so I have no risk.” The sun is the main factor, but not the only one.
Sources
- American Academy of Dermatology. Guidelines of care for the management of primary cutaneous melanoma. Journal of the American Academy of Dermatology, 2019. https://www.jaad.org/article/S0190-9622(18)32588-X/fulltext
- Garbe C., Amaral T., Peris K. et al. European consensus-based interdisciplinary guideline for melanoma. Part 1: Diagnostics — Update 2024. European Journal of Cancer, 2024. https://www.sciencedirect.com/science/article/pii/S0959804924017593
- Primary Care Dermatology Society (PCDS). Melanoma — Clinical Guidelines, 2025. https://reference.medscape.com/cc1/p10/key-learning-points-pcds-melanoma-2025a100095a
- DermNet NZ. ABCDEFG of melanoma. https://dermnetnz.org/topics/abcdes-of-melanoma
- National Cancer Registry of Ukraine. Bulletin “Cancer in Ukraine.” http://www.ncru.inf.ua/publications/
- Unified clinical protocol for primary, secondary — specialized — and tertiary — highly specialized — medical care “Cutaneous melanoma.” Order of the Ministry of Health of Ukraine No. 784 dated 27.11.2015. https://www.dec.gov.ua/wp-content/uploads/2019/11/2015_784_ykpmd_melanoma.pdf
- Tan W.P., Jansen S., Stern J.B. Subungual Melanoma. StatPearls Publishing, 2024. https://pubmed.ncbi.nlm.nih.gov/29494087/
- Baran R., Kechijian P. Hutchinson’s sign: a reappraisal. Journal of the American Academy of Dermatology, 1996. https://pubmed.ncbi.nlm.nih.gov/8543700/
- Maymone M.B.C., Greer R.O., Burdine L.K. et al. Differential Diagnosis of Pigmented Lesions in the Oral Mucosa. Cancers, 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11240708/
- Pizzichetta M.A., Talamini R., Stanganelli I. et al. Amelanotic/hypomelanotic melanoma: clinical and dermoscopic features. British Journal of Dermatology, 2004. https://pubmed.ncbi.nlm.nih.gov/15214902/
- Robinson J.K. Skin check partner assistance for melanoma skin self-examination by at-risk patients. Future Oncology, 2020. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7273363/
- U.S. Preventive Services Task Force. Screening for Skin Cancer: Recommendation Statement. JAMA, 2023. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/skin-cancer-screening


